
Document Contents
The revision of these entry-level competencies would not have been possible without the assistance of several people. The Registered Psychiatric Nurse Regulators of Canada (RPNRC) would like to thank the psychometric team at Meazure Learning (Yardstick Assessment Strategies Inc.) and the members of the Subject Matter Expert (SME) working group who committed their time, knowledge and experience to the preparation of numerous drafts and revisions of this document.
We are very grateful to the RPNs, RPN regulatory authorities, the educational community and employers for their invaluable time and effort assisting us in validating these competencies.
The RPNRC approved these entry-level competencies as the Entry Level Competencies for Registered Psychiatric Nurses in Canada on February 12, 2025. These entry-level competencies were subsequently approved and adopted by the RPN regulatory authorities in Canada.
This document replaces the RPN Entry-Level Competencies document published in 2014.
The College of Registered Psychiatric Nurses of Alberta approved the 2025 entry-level competencies for the Registered Psychiatric Nurses on March 1, 2025.
Copyright © 2025 RPNRC
All rights reserved. The reproduction, storage in a retrieval system or transmission in any form or by any means (including electronic, mechanical, photographic, photocopying or recording) of any part of this publication without the prior written permission from RPNRC (Registered Psychiatric Nurse Regulators of Canada) is an infringement of copyright law.
Public release date
May 29, 2025
Adopted by the College of Registered Psychiatric Nurses of Alberta
Provincial Council March 1, 2025.
The Registered Psychiatric Nurse Entry-Level Competencies are revised every five to seven years at a national level to ensure they are relevant to Registered Psychiatric Nurse (RPN) practice, consistent among the jurisdictions, and support workforce mobility requirements of the Canadian Agreement on Internal Trade. In February 2024, the Registered Psychiatric Nurse Regulators of Canada (RPNRC) contracted with Meazure Learning (Yardstick Assessment Strategies Inc.) to review and update the RPN Entry-Level Competencies (ELCs). The review process included consultation with each of the regulatory bodies that regulate RPNs, as well as with RPNs from a variety of practice settings, psychiatric nursing faculty and clinical educators, and employers.
This document replaces the RPN Entry-Level Competencies document published in 2014.
Registered Psychiatric Nurses (RPNs) are autonomous professionals. The core of psychiatric nursing practice is therapeutic communication and the therapeutic relationship. Emotion, behaviour and cognition are a major focus in psychiatric nursing practice. Many psychotherapeutic interventions are performed through the psychiatric nurse’s interaction with the client (Kunyk et al., 2023).
RPNs focus on mental and neurodevelopmental health, mental illness and addictions and use the nursing process and bio-psycho-social and spiritual models of assessment for a holistic approach to care. Entry level RPNs are also prepared with a foundational knowledge of nursing and medical-surgical nursing practice. The profession is committed to the prevention of illness and to the promotion and maintenance of optimal health, rehabilitation and recovery.
Psychiatric nursing education programs prepare entry-level RPNs to begin their practice in a variety of practice settings, with diverse populations, and across the lifespan. The practice environment plays a crucial role in the further development and consolidation of the entry-level competencies. Employers are integral in supporting entry level RPNs to further develop their competencies through orientation, continuing education and professional-development opportunities.
The 2025 Registered Psychiatric Nurse Competencies reflect the foundational knowledge, skills, judgments and attitudes required of RPNs in order to provide safe, competent, ethical and compassionate care. The entry-level competencies are used by the regulatory bodies, psychiatric nursing education programs and other external partners for several purposes, including but not limited to:
- Curriculum development
- Psychiatric nursing education program review and approval
- Development of the Registered Psychiatric Nurses of Canada Examination (RPNCE) Development of standards
- Competency-based and/or practice assessments for initial or returning applicants (including internationally educated RPNs and current registrants)
- Practice consultations Professional conduct review
- Information for public, employers and external partners
Indigenous-specific racism1 in the Canadian health care system has persisted since its inception and continues to this day. The Registered Psychiatric Nurse Regulators of Canada (RPNRC) acknowledge that systemic racism and discrimination towards Indigenous Peoples adversely impact Indigenous Peoples’ access to, and treatment in, health services. The Regulators believe that Indigenous-specific racism is unacceptable in our society and condemn racist attitudes and behaviours among health care professionals, and denounce systemic racism within health care institutions, structures and policies.
RPNs have a responsibility to address racism and bias at the individual and system levels. RPNs are expected to provide culturally safe care and actively embrace cultural humility; they are also called upon to recognize and address power imbalances in the health care system. Adopting reflective practice allows RPNs to understand personal and systemic biases and acknowledge the experience of others.
The RPNRC expects that the Entry-Level Competencies for Registered Psychiatric Nurses will support RPNs in playing a key role in addressing anti-Indigenous racism in health care.
1 "Anti-Indigenous racism" is the terminology used by the Government of Canada. The terms "Indigenous-specific racism" and "anti-Indigenous racism" can be used interchangeably.
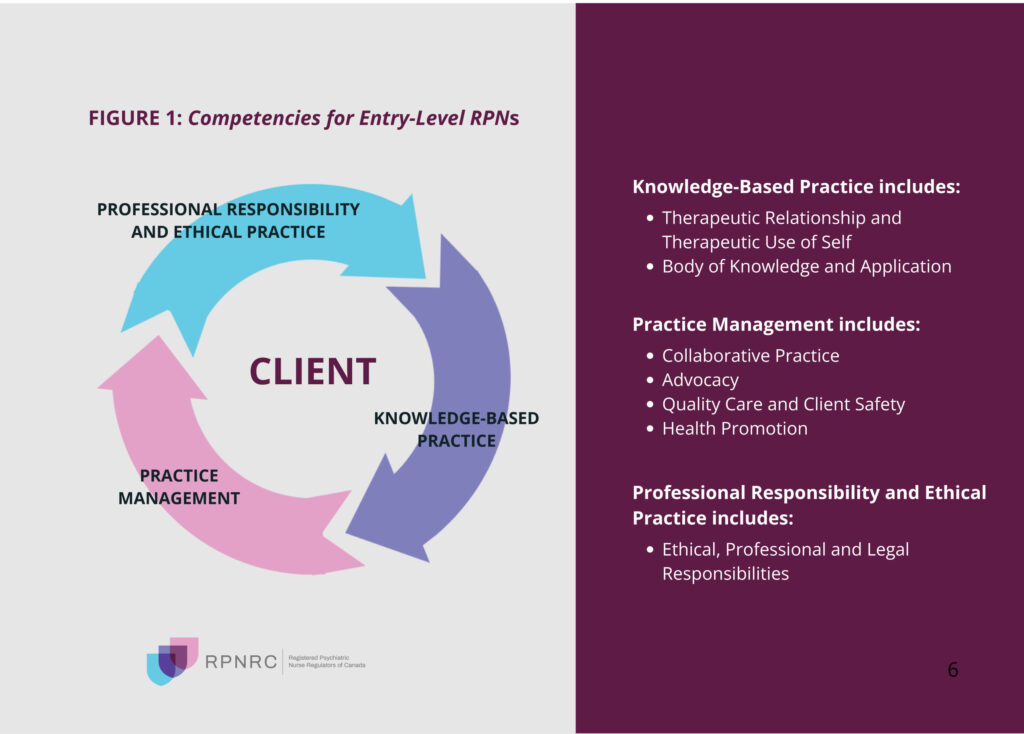
The competency framework chosen by the Registered Psychiatric Nurse (RPN) profession in Canada is an adaptation of the client-centred framework (see Figure 1). The basis for using this framework is the client-centred approach of psychiatric nursing practice.
Although the RPN profession has chosen a client-centred framework over a role-based one, the practice of psychiatric nursing occurs in the domains of direct practice,education, research and administration. Roles with respect to communication, advocacy, collaboration, and leadership are embedded in the entry-level competencies and within the chosen organizing framework.
These principles apply to the education and practice of entry-level registered psychiatric nurses.
The Entry-Level Registered Psychiatric Nurse (RPN):
- Is a beginning practitioner. It is unrealistic to expect an entry-level RPN to function at the level of practice of an experienced RPN.
- Practices within a legislative framework, practice standards, ethics and the RPN scope of practice in their jurisdiction.
- Seeks guidance from reliable sources when they encounter situations outside their competence.
- Possesses specialized knowledge in mental health, mental illnesses, neurodevelopmental disabilities, and substance-related and addictive disorders that integrates communication, psychology, sociology, psychopharmacology, psychiatric nursing theory, research, and mental health law and ethics.
- Has a foundational knowledge of the biological and nursing sciences and possesses a range of general medical and surgical nursing competencies.
- Applies critical thinking, problem solving, clinical reasoning and judgment in their professional practice.
- Practices safely, competently and ethically in situations of health and illness and with clients across the lifespan, including individuals, families, groups and communities.
- Applies competencies across all practice settings, even if their psychiatric nursing education program did not expose them to all practice environments or client types.
- Continues to consolidate theoretical and experiential learning through collaboration, mentoring and support from the interdisciplinary team.
- Practices collaboratively and assumes formal and informal leadership roles.
This document includes words specific to psychiatric nursing that may not be familiar to all readers. Some words (e.g., "psychotherapy") have no universally accepted definitions. Please see the Glossary for specialized words used in this document.
Knowledge-Based Practice
1. THERAPEUTIC RELATIONSHIPS AND THERAPEUTIC USE OF SELF
Therapeutic use of self is foundational to the therapeutic relationship that Registered Psychiatric Nurses have with clients.
1.1 Apply therapeutic use of self to inform all areas of psychiatric nursing practice.
1.1.1 Engage in a deliberate and ongoing process of self-awareness to establish and sustain client-centred relationships.
1.1.2 Assess, evaluate, and act to ensure the influences of one’s personal beliefs, values, thoughts, motivations, biases and limitations on client interactions.
1.1.3 Establish and maintain boundaries within a therapeutic relationship.
1.1.4 Recognize, identify and validate the emotions and experiences of others.
1.1.5 Recognize and address the impact of transference and countertransference in the therapeutic relationship.
1.1.6 Demonstrate unconditional positive regard, empathy and congruence in relationships.
1.1.7 Monitor and adapt the communication process by using a range of verbal and non- verbal strategies to ensure effective interactions.
1.1.8 Evaluate the effectiveness of therapeutic use of self on others.
1.1.9 Engage in personal and professional development activities to enhance the therapeutic use of self.
1.1.10 Engage in self-assessment and self-care activities to manage secondary trauma, vicarious trauma and compassion fatigue.
1.2 Establish a therapeutic relationship with the client
1.2.1 Develop a rapport and promote trust through mutual respect, genuineness, empathy, acceptance and collaboration.
1.2.2 Establish and negotiate boundaries to clarify the nature, content and limits of the therapeutic relationship.
1.2.3 Engage with the client using a strengths-based approach to explore goals, learning and growth needs.
1.2.4 Differentiate between therapeutic and non-therapeutic communication techniques.
1.2.5 Apply therapeutic communication strategies and techniques to reduce emotional distress, facilitate cognitive and behavioural change and foster growth.
1.3 Maintain the therapeutic relationship.
1.3.1 Engage in ongoing assessment, planning, implementation and evaluation over the course of the therapeutic relationship.
1.3.2 Collaborate with the client to help achieve client-centred goals.
1.3.3 Adapt therapeutic strategies as necessary when encountering resistance and ambivalence.
1.3.4 Provide psychoeducation to client and evaluate learning.
1.3.5 Evaluate strengths, resiliency, problems and goals and redefine them with the client as necessary.
1.3.6 Evaluate the impact of transference and countertransference in the therapeutic relationship.
1.3.7 Engage in collaborative consultation to facilitate, support and enhance the therapeutic use of self.
1.4 Terminate the therapeutic relationship.
1.4.1 Identify the end point of the therapeutic relationship.
1.4.2 Summarize the outcomes of the therapeutic relationship with the client.
1.4.3 Evaluate the therapeutic process and outcomes of the interventions.
1.4.4 Establish the boundaries of the post-therapeutic relationship.
1.4.5 Determine the need for follow-up and establish referral(s) or transfer care accordingly.
2. Body Of Knowledge And Application
Registered Psychiatric Nurses’ practice is comprised of foundational nursing, medical- surgical nursing and specialized psychiatric nursing knowledge. RPNs use critical inquiry and apply a decision-making process in all domains of psychiatric nursing practice.
Evidence Informed Knowledge
2.1 Demonstrate knowledge of the health sciences, including anatomy, physiology, microbiology, nutrition, pathophysiology, palliation, psychopharmacology, pharmacology, epidemiology, genetics, sexual and reproductive health, and prenatal and genetic influences on development.
2.2 Demonstrate knowledge of social sciences and humanities, including psychology, psychopathology, psychotherapy, sociology, human growth and development, neurodevelopment, communication, leadership, statistics, research methodology, philosophy, ethics, spiritual care, determinants of health and primary health care.
2.3 Demonstrate knowledge of nursing science, conceptual nursing models, nursing skills, procedures and interventions.
2.4 Demonstrate knowledge of current and emerging health issues across the lifespan and in all settings.
2.5 Demonstrate knowledge of community, global and population health issues, including the determinants of health.
2.6 Demonstrate knowledge of the relationship between Indigenous and western knowledge systems and how determinants of health are linked to Indigenous health and mental health outcomes.
2.7 Demonstrate knowledge of Indigenous cultural rights, values and practices and recognize the knowledge shared by Indigenous Peoples.
2.8 Demonstrate knowledge of the concepts of equity , diversity and inclusion and how determinants of health are linked to health and mental health outcomes.
2.9 Demonstrate knowledge of informatics and emerging technologies.
2.10 Demonstrate evidence-informed knowledge of psychopathology across the lifespan.
2.10.1 Demonstrate knowledge of disorders of neurodevelopmental health and mental health.
2.10.2 Demonstrate knowledge of screening and diagnostics (e.g., standardized assessment scales, Diagnostic and Statistical Manual of Mental Disorders).
2.10.3 Demonstrate knowledge of psychiatric and psychosocial interventions.
2.11 Demonstrate evidence-informed knowledge of substance-related and addictive disorders
2.11.1 Demonstrate knowledge of substance-related and addictive disorders.
2.11.2 Demonstrate knowledge of screening and diagnostics.
2.11.3 Demonstrate knowledge of medical, psychosocial, and psychiatric interventions.
2.12 Demonstrate evidence-informed knowledge of co-occurring disorders.
2.13 Demonstrate evidence-informed knowledge of pathophysiology across the lifespan.
2.13.1 Demonstrate knowledge of medical disorders.
2.13.2 Demonstrate knowledge of laboratory tests and other diagnostics.
2.13.3 Demonstrate knowledge of medical-surgical interventions.
2.14 Demonstrate knowledge of therapeutic modalities.
2.15 Demonstrate knowledge of how complementary or alternative therapies can impact treatment.
2.16 Demonstrate knowledge of recovery models.
2.17 Demonstrate knowledge of trauma and violence-informed care.
2.18 Demonstrate knowledge of the impact of social, cultural, family, environmental, and systemic factors on health outcomes.
2.19 Demonstrate knowledge of the impact of colonialism on the health outcomes of Indigenous Peoples.
2.20 Demonstrate knowledge of the dynamics of interpersonal abuse (e.g., child abuse, intimate partner violence, elder abuse).
2.21 Demonstrate knowledge of mental health legislation and other relevant legislation.
Application of Body of Knowledge
2.22 Conduct a holistic client assessment.
2.22.1 Use an evidence-informed client-focused framework to guide practice.
2.22.2 Obtain informed consent from the client when required, ensuring they understand the scope and nature of the intervention.
2.22.3 Perform a holistic health and social assessment.
2.22.4 Perform a comprehensive or focused physical health assessment.
2.22.5 Perform an in-depth mental health assessment.
2.22.6 Incorporate data from other sources (e.g., laboratory tests, collateral information, diagnostics).
2.22.7 Assess the ethical and legal implications of interventions before providing care.
2.23 Formulate a clinical judgment based on the assessment data.
2.23.1 Identify clinical indicators that are commonly associated with psychiatric disorders, neurodevelopmental disorders, and substance-related and addictive disorders using current nomenclature (e.g., Diagnostic and Statistical Manual of Mental Disorders).
2.23.2 Identify clinical indicators that are commonly associated with medical disorders.
2.23.3 Use critical thinking to analyze and synthesize data collected.
2.23.4 Use diagnostic reasoning to formulate a psychiatric nursing diagnosis.
2.23.5 Use diagnostic reasoning to assess the appropriateness of pharmacological and psychopharmacological interventions.
2.24 Collaborate with the client to develop a holistic and client-centred plan to address identified problems, minimize the development of complications and promote optimal functioning and quality of life.
2.24.1 Discuss client-directed goals to identify interventions that promote health, prevent illness, reduce harm and foster recovery.
2.24.2 Recommend a plan of care that promotes client responsibility, autonomy and independence to the greatest extent possible.
2.25 Implement evidence-informed interventions with the client, according to the plan of care.
2.25.1 Provide psychiatric nursing and psychosocial interventions (e.g., cognitive behavioural therapy; individual, group and family psychotherapy; crisis interventions; somatic therapies).
2.25.2 Perform nursing interventions to address medical conditions and the client’s physical health needs (e.g., intravenous therapy, nutrition therapy, infection prevention and control, ventilation, skin and wound care, pre- and post-operative care).
2.25.3 Integrate knowledge of pharmacology and psychopharmacology for safe medication administration.
2.25.4 Determine the need for referrals and liaise to promote access to resources that can optimize health outcomes and meet client-centred goals.
2.26 Use critical thinking and clinical judgment to determine the level of risk and coordinate effective interventions for emergencies.
2.26.1 Apply crisis intervention skills with clients experiencing acute emotional, physical, behavioural, and mental distress.
2.26.2 Conduct ongoing suicide, homicide and violence risk assessments and apply interventions.
2.26.3 Intervene to minimize agitation and aggression, de-escalate and manage behaviour in the least restrictive manner.
2.26.4 Intervene to prevent self-harm or minimize injury related to self-harm.
2.26.5 Recognize and intervene to stabilize clients experiencing medical emergencies.
2.26.6 Evaluate the effectiveness and appropriateness of the plan of care.
2.26.7 Collect, analyze and synthesize data to evaluate the outcomes from the plan of care.
2.26.8 Use a critical inquiry process to continuously monitor the effectiveness of client care in relation to anticipated outcomes.
2.26.9 Modify the plan of care in collaboration with the client and according to evaluation findings.
Practice Management
3. COLLABORATIVE PRACTICE
Registered Psychiatric Nurses work in collaboration with clients, multidisciplinary and interdisciplinary teams, and internal and external partners to deliver comprehensive psychiatric nursing care.
3.1 Establish and maintain relationships that foster continuity and client-centred care, whether a formalized team exists.
3.1.1 Seek out the input and engagement of clients and value them as partners.
3.1.2 Foster communication between the client and others involved in care delivery to support effective partnerships.
3.1.3 Be transparent when communicating information with clients.
3.1.4 Share relevant information with multidisciplinary and interdisciplinary teams, as well as internal and external partners.
3.1.5 Promote collaborative, shared and evidence-informed decision making.
3.2 Partner effectively with team members in the coordination and delivery of client-centred care.
3.2.1 Demonstrate an understanding of the roles, responsibilities and perspectives of client, teams, and partners.
3.2.2 Communicate the roles and responsibilities of the RPN to client, team members, and partners.
3.2.3 Demonstrate when to assume a leadership role, when to take a supportive role and when to refer or consult.
3.2.4 Assume leadership responsibilities for coordinating care.
3.2.5 Identify and mitigate barriers to care in order to enhance health care outcomes.
3.3 Share responsibility for resolving conflict with team members.
3.3.1 Foster a safe, respectful environment where diverse perspectives can be shared, and conflicts are addressed constructively.
3.3.2 Recognize actual or potential conflict situations; address and resolve disagreements,including analyzing the causes; and work to reach an acceptable, cooperative solution.
4. ADVOCACY
Registered Psychiatric Nurses engage systems and individuals to support and empower clients to advance their health and well-being.
4.1 Collaborate with clients to act on issues that may impact their health and well-being.
4.1.1 Advocate for resources that enhance the client’s quality of life and social inclusion.
4.1.2 Inform clients of their rights and options.
4.1.3 Support the client’s right to evidence-informed decision making.
4.1.4 Support client autonomy, right to choice, and right to live at risk.
4.1.5 Advocate for the least restrictive treatment options and environments.
4.2 Promote awareness of mental health, mental illness, and addictions by providing accurate information and challenging negative attitudes and behaviours that contribute to stigma and discrimination.
4.2.1 Demonstrate knowledge and understanding of demographic and socio-political environments.
4.2.2 Recognize the impact of mental illness, stigma and discrimination on individuals, families, groups and communities.
4.2.3 Recognize and address attitudes and behaviours that contribute to stigma and discrimination.
4.2.4 Provide education about mental health, mental illness, neurodevelopmental disorders, and substance-related and addictive disorders.
4.2.5 Engage with key partners and the community to promote mental health and wellness.
4.2.6 Engage in addressing social justice issues at an individual or community level.
4.3 Promote awareness of and challenge discrimination based on race, ethnicity, culture, political or spiritual beliefs, social or marital status, gender, gender identity, gender expression, sexual orientation, age, health status, place of origin, lifestyle, mental or physical ability, socio-economic status or any other attribute.
4.3.1 Demonstrate knowledge and understanding of the application of the principles of equity, diversity and inclusion.
4.3.2 Recognize attitudes and behaviours of self and others that contribute to unconscious bias.
4.3.3 Recognize factors that contribute to racism and discrimination in health care.
4.4 Advocate for the use of Indigenous health knowledge and healing practices in collaboration with Indigenous healers, Elders and Knowledge Keepers, and communities.
4.5 Foster a culture of trust, mutual respect and open communication to address racism and discrimination
4.5.1 Implement anti-racism and anti-discrimination practices, including Indigenous-specific anti-racism.
5. QUALITY CARE AND CLIENT SAFETY
Registered Psychiatric Nurses enhance the safety, quality and effectiveness of psychiatric nursing practice through leadership and collaboration.
5.1 Use reflective practice and evidence to guide one’s psychiatric nursing practice.
5.1.1 Reflect on and critically analyze practice to inform and enhance future practice.
5.1.2 Reflect on current evidence and research from various sources and determine relevance to client need and practice setting.
5.1.3 Integrate research findings and evidence-informed practices to optimize health outcomes.
5.1.4 Evaluate the safety, quality and effectiveness of practice.
5.2 Integrate continuous quality improvement principles and activities into psychiatric nursing practice.
5.2.1 Collaborate in developing, implementing and evaluating policies, procedures and activities that promote quality care and client safety.
5.2.2 Recognize, report and document potential risks, hazards and opportunities to improve practices.
5.2.3 Identify and address occupational hazards and psychological harms related to exposure to violence and trauma in health care.
5.2.4 Implement interventions to address potential risks and hazards. Take action to prevent or minimize harm from unsafe practices.
5.2.5 Evaluate the effectiveness of continuous quality improvement interventions in practice.
5.3 Integrate cultural awareness, safety and sensitivity into practice.
5.3.1 Self-reflect on personal beliefs, biases, values and attitudes and how they impact one’s practice.
5.3.2 Implement strategies to mitigate the impact of personal beliefs, biases, values and attitudes on client care.
5.3.3 Explore the client’s cultural needs, beliefs, practices and preferences.
5.3.4 Incorporate the client’s cultural preferences and personal perspectives into the plan and delivery of care.
5.3.5 Engage in opportunities to learn about various cultures and beliefs and the health practices of a particular group, community or society.
5.3.6 Incorporate knowledge of culture and how intersectionality and multiple identities shape one’s life experience and contribute to health outcomes.
5.3.7 Acknowledge historical injustices and address power imbalances and systemic barriers that negatively impact the health outcomes of Indigenous Peoples.
6. HEALTH PROMOTION
Registered Psychiatric Nurses use their expertise to promote the physical and mental health of clients to prevent disease, illness and injury.
6.1 Engage in health promotion and the prevention of disease, illness and injury.
6.1.1 Integrate knowledge of the determinants of health, health disparities, and health inequities when assessing health promotion needs.
6.1.2 Develop and implement evidence-informed health promotion strategies and programs based on a range of theories and models.
6.1.3 Select and implement evidence-informed interventions to promote health and prevent disease, illness and injury.
6.1.4 Engage clients to seek out or identify resources that promote health.
6.1.5 Contribute to the development of policies and standards that support health promotion and prevent disease, illness and injury.
6.1.6 Advocate for health promotion within the health care systems and environments.
6.2 Engage in health and mental health promotion when collaborating with clients.
6.2.1 Integrate knowledge of determinants of health in the assessment process.
6.2.2 Recognize the interrelationship of comorbid physical and mental health and addictions issues and their impact on overall health.
6.2.3 Assess the biological, psychological, social, spiritual, cultural and environmental risk and protective factors specific to health and mental health.
6.2.4 Incorporate strategies into health care planning that strengthen protective factors and enhance resilience.
6.2.5 Contribute to the development of policies and standards that support health and mental health promotion.
6.3 Engage in the prevention of mental illness, neurodevelopmental disorders and substance-related and addictive disorders when collaborating with clients.
6.3.1 Use a variety of strategies to address stigma and discrimination around mental illness, neurodevelopmental disorders and substance-related and addictive disorders.
6.3.2 Recognize and address the impact of societal factors that contribute to mental illness, neurodevelopmental disorders and substance-related and addictive disorders.
6.3.3 Incorporate strategies into health care planning that reduce risk.
6.3.4 Incorporate trauma and violence-informed philosophies and evidence-informed practices into health care planning.
6.3.5 Implement intervention to promote insight into the relationship between mental illness and addictive disorders.
6.3.6 Integrate harm-reduction strategies and evidence-informed practices into health care planning.
6.3.7 Engage and empower clients to seek out and/or identify resources for addiction treatment and recovery.
6.3.8 Contribute to the development of policies and standards that support the prevention of mental illness and addictive disorders.
6.3.9 Implement suicide prevention strategies when collaborating with clients who are at risk for suicide.
6.3.10 Collaborate with communities in suicide prevention and postvention activities.
Professional Responsibility and Ethical Practice
7. ETHICAL, PROFESSIONAL AND LEGAL RESPONSIBILITIES
Registered Psychiatric Nurses practice within legal requirements, demonstrate professionalism and uphold professional codes of ethics, standards of practice, bylaws and policies.
7.1 Practice in compliance with federal and provincial/territorial legislation and other legal requirements.
7.1.1 Demonstrate knowledge of the legislation governing psychiatric nursing practice.
7.1.2 Adhere to the psychiatric nursing code of ethics, standards of practice and bylaws of the regulatory authority.
7.1.3 Practice within the jurisdiction’s legislated scope of practice, standards, limits and conditions.
7.1.4 Adhere to and apply the jurisdiction’s mental health legislation.
7.1.5 Adhere to and apply other relevant legislation that has an impact on practice.
7.1.6 Protect client confidentiality and adhere to relevant legislation that governs the privacy, access, use, retention and disclosure of personal information.
7.1.7 Adhere to legal requirements regarding client consent.
7.1.8 Adhere to any legislated duty to report, including the duty to report abuse or to report unprofessional or unsafe practice or the risk of such.
7.1.9 Adhere to standards and policies regarding documentation, including being timely, accurate, clear, concise and legible.
7.2 Assume responsibility for upholding the requirements of professional regulation in the interest of public protection.
7.2.1 Accept responsibility for own actions, decisions and professional conduct.
7.2.2 Practice within own level of competence and use professional judgment when accepting responsibilities, including seeking out additional information or guidance when required.
7.2.3 Demonstrate an understanding of professional regulation.
7.2.4 Engage in a process of continuous learning and self-evaluation, including following the requirements of the regulatory authority’s continuing competence program or continuing education program.
7.2.5 Demonstrate an understanding of fitness to practice in the context of public protection and strive to maintain a level of personal health, mental health and well-being in order to provide safe, competent and ethical care.
7.2.6 Question and act when policies, orders, decisions or actions are unclear or inconsistent with positive client outcomes, best practices, health and safety standards or client goals.
7.3 Demonstrate a professional presence and model professional behaviour.
7.3.1 Conduct oneself in a manner that promotes a positive image of the profession.
7.3.2 Respond professionally, regardless of the behaviour of others.
7.3.3 Articulate the role and responsibilities of a RPN.
7.3.4 Exercise professional judgment when agency policies and procedures are unclear or absent.
7.3.5 Organize and prioritize workload and develop time-management skills for meeting responsibilities.
7.3.6 Demonstrate professional leadership.
7.3.7 Maintain professional boundaries in the use of technology, electronic communication and social media.
7.4 Uphold and promote the ethical values of the profession.
7.4.1 Conduct oneself in a manner that reflects honesty, integrity, reliability and impartiality.
7.4.2 Avoid situations that could give rise to potential, actual, or perceived conflicts of interest and ensure that the vulnerabilities of others are not exploited for one’s own interest.
7.4.3 Identify the effects of one’s own values, beliefs, biases and assumptions on decision making and interactions with clients and other members of the health care team.
7.4.4 Recognize ethical dilemmas and implement steps toward a resolution.
7.4.5 Differentiate between personal and professional relationships and maintain the boundaries of the psychiatric nurse–client relationship.
Anti-Racism Practices: The practice of becoming actively conscious about race and racism, opposing racism and promoting equality. The primary goal is to dismantle structures and behaviours that perpetuate racial inequalities and to create environments where all racial and ethnic groups are treated with dignity and respect.
Anti-Discrimination Practices: The policies, guidelines, and actions to prevent and address the unfair treatment of individuals based on characteristics such as race, gender, age, religion, sexual orientation, disability or other protected categories. These practices aim to promote equality, inclusion and fairness by ensuring that everyone has equal opportunities and is not subjected to bias or prejudice.
Client: The client may be an individual, family, group, community or population.
Clinical Judgement: an interpretation or conclusion about a client’s needs, concerns, or health problems, and/or the decision to take action (or not), use or modify standard approaches, or improvise new ones as deemed appropriate by the client’s response (Tanner, 2006). Clinical judgment in nursing is multifaceted and involves both experiential knowledge as well as evidence-based knowledge (Hussein, Olfert, & Hakkola, 2022).
Collaborative Consultation: an interactive and ongoing process in which professionals with different expertise, knowledge, or experience voluntarily work together to enhance client care. Collaborative consultation is characterized by mutual trust, respect, and open communication amongst professionals who may be from the same or different disciplines (adapted from Robinson, 1991 and the Canadian Interprofessional Health Collaborative, n.d.).
Collaborative Practice: In health care, collaborative practice occurs when multiple health workers from different professional backgrounds provide comprehensive services by working with clients, their families, carers and communities to deliver the highest quality of care across settings. Practice includes both clinical and nonclinical health-related work, such as diagnosis, treatment, surveillance, health communications and management (World Health Organization, 2010).
Compassion Fatigue: A condition characterized by emotional and physical exhaustion. Compassion fatigue results from being regularly exposed to other people’s trauma and suffering and can lead to a decrease in the RPN’s effectiveness in their work (Jones & Beauvais, 2023). Compassion fatigue falls within the category of “empathy-based” stress outcomes for caregivers (Heber et al., 2023).
Competencies: The integrated knowledge, skills, judgment and attitudes required by an RPN to practice competently, ethically and safely (Moghabghab et al., 2018).
Congruence: Alignment of the RPN’s internal experiences and outward expression within an encounter. Congruence contributes to authenticity and genuineness within the therapeutic relationship.
Consent: Consent to health care means having the right to choose, refuse or revoke health care after being informed about the proposed plan of care. Consent is based on a legal requirement, as well as respect for clients’ rights to enough information to make decisions about their health care (BCCNM, 2016).
Countertransference: All of the registered psychiatric nurse’s feelings and attitudes toward the client. Feelings and perceptions caused by countertransference may interfere with the RPN’s ability to understand the client (Kunyk et al., 2023).
Critical Thinking: The deliberate, reflective process used by RPNs to assess situations, make decisions and solve problems. It involves analyzing information, evaluating evidence and considering different perspectives to provide safe and effective care.
Culture: The shared beliefs, values and practices of a group that shape group members’ thinking and behaviour in patterned ways. Culture can also be viewed as a blueprint for guiding actions that impact care, health and well-being (Government of Canada, 2013).
Determinants of Health: The health of individuals is determined by a person’s social and economic factors, the physical environment and the person’s individual characteristics and behaviour.
Determinants include income and social status; social support networks; education and literacy; employment/working conditions; social environments; physical environments; personal health practices and coping skills; healthy child development; biology and genetic endowment; health services; gender; and culture (Governement of Canada, 2013).
Equity, Diversity and Inclusion: The principles of equity, diversity and inclusion are intertwined; they are defined by the process of improving the terms of participation in a discussion (inclusion) and promoting and integrating diverse perspectives (diversity), in order to attain fair access to opportunities (equity) (McGill University, 2024).
Evidence-Informed Decision Making: An approach which emphasizes that decisions should be informed by the best available evidence from research, with consideration of factors such as context, public opinion, effectiveness, safety, impact on equity, feasibility of implementation, affordability, sustainability, and acceptability to clients and the public (adapted from the Pan American Health Organization, 2022).
Harm-Reduction: An approach to public health which focuses on reducing the harm associated with risky behaviours. The approach can be applied to substance use, gambling, high-risk sexual activity and other behaviours that present risk. It recognizes that some people may not be ready, willing or able to stop the behaviour completely and, therefore, in some cases, finding ways to reduce the harmful effects of the risk on the person, their family and the community is a more realistic approach (Centre for Addictions and Mental Health, 2024).
Health Promotion: The process of enabling people to increase control over, and to improve, their health. It moves beyond a focus on individual behaviour toward a wide range of social and environmental interventions (World Health Organization, 2024a).
Holistic: Characterized by the treatment of the whole person, taking into account mental and social factors, rather than just the symptoms of an illness.
Indigenous Peoples: "Indigenous Peoples" is a collective name for the original peoples of North America and their descendants. The Canadian Constitution recognizes three distinct groups of Indigenous (Aboriginal) Peoples: Indians (referred to as First Nations), Métis and Inuit. Increasingly, and in keeping with international agreements, “Indigenous Peoples” is being used instead of “Aboriginal peoples.” (Government of Canada, 2024).
Intersectionality: A framework that describes how people’s overlapping social identities relate to social structures of racism and oppression (University of British Columbia, 2021).
Judgment: The evaluation of evidence to a make a clinical decision. In the context of psychiatric nursing, it includes the initial reaction of the RPN to the client. It is the ability to make critical distinctions and achieve a balanced viewpoint.
Leadership: The effort by leaders who may, but do not necessarily, hold formal positions of authority to engage followers in the joint pursuit of mutually agreed-upon goals (Kellerman, 1999).
Mental Health Promotion: an approach to cultivate positive mental health in individuals and communities through a combination of targeted and broad interventions across the life course, in communities, workplaces, and schools. It is distinct from (but intersects with) prevention, which aims to reduce symptoms and rates of mental illness. Mental health promotion initiatives build individual skills, supportive environments, and community resilience, all of which are recognized as integral to the development of mentally healthy societies. What makes mental health promotion unique is its attentiveness to health and social systems as well as its focus on individual and population health. Mental health promotion efforts are numerous and fall into several broad categories: information dissemination, anti-stigma/discrimination reduction campaigns, health risk appraisals or wellness assessments, lifestyle and behavioural change, and environmental control. They may be universal (developed for an entire group/population), selective (targeted at those identified as at risk) or indicated (developed for those expressing early signs or symptoms of mental health problems).
Mental health promotion efforts aim to develop positive mental health among all people, whether they live with or without a mental illness (Canadian Mental Health Association, 2019).
Occupational Hazards: Any source of potential damage or harm to someone or something within the workplace (Canadian Centre for Occupational Health and Safety, 2024).
Postvention: An intervention conducted after a crisis event, largely taking the form of support for those affected by the event.
Primary Health Care: A whole-of-society approach to effectively organize and strengthen national health systems to bring services and the attainment of well-being closer to communities. It has three components: integrated health services to meet people’s health needs throughout their lives; addressing the broader determinants of health through multisectoral policy and action; and empowering individuals, families and communities to take charge of their own health (World Health Organization, 2024b).
Psychiatric Nursing Diagnosis: Identification of an illness or health issue by examination and analysis of the client’s signs and symptoms.
Psychoeducation: An evidence-based intervention aimed at educating people about their illness and its management, empowering clients to cope more effectively with their condition (Hedman-Lagerlof & Axelsson, 2019; Jones & Beauvais, 2023).
Psychopharmacology: The study and use of drugs that influence thinking, behaviour, or emotion (Thomas, 2021).
Psychotherapy: Treatment that focuses on the emotional problems expressed by the client, for the purpose of changing behaviour related to the cognitive, affective and behavioural functions and to promote insight, empathy and control. Clinicians who engage in psychotherapy use a variety of modalities and techniques and work within many different frameworks and theories to promote change. Psychotherapy may be a brief or long-term process that is centred on the depth of the relationship between the client and therapist and the therapeutic alliance.
Recovery: Living a satisfying, hopeful and meaningful life, even when there may be ongoing limitations related to mental health problems and illnesses. It starts with the fundamental belief that not only is recovery possible, it should be expected regardless of diagnosis or situation (Mental Health Commission of Canada, 2016).
Recovery Model: A client-centred approach that stresses hope, living a full and productive life and eventual recovery. Clients partner with health care providers and aim to extend their improvement beyond stability (Government of Canada, 2013).
Reflective Practice: A cognitive skill that demands that practitioners make a conscious effort to look at a situation with an awareness of their own beliefs, values, and practice, thereby enabling them to learn from experiences and incorporate that learning toward improving client care outcomes. It also leads to knowledge development in nursing (Patel & Metersky, 2022).
RPN Regulatory Authorities: In Canada, the psychiatric nursing regulatory authorities are comprised of the British Columbia College of Nurses and Midwives (BCCNM), College and Association of Nurses of the Northwest Territories and Nunavut (CANNN), College of Registered Nurses and Midwives of Prince Edward Island (CRNMPEI), College of Registered Psychiatric Nurses of Alberta (CRPNA), the College of Registered Psychiatric Nurses of Manitoba (CRPNM) and the College of Registered Psychiatric Nurses of Saskatchewan (CRPNS). The Government of Yukon also regulates RPNs.
Secondary Trauma: A mental health condition that may occur as a result of indirect exposure to details of one or more potentially psychologically traumatic events in the course of professional duties such as hearing the content of psychologically traumatic events experiences from clients. Secondary traumatic stress is an occupational hazard of first responders, trauma care workers, and health care professionals who work with traumatized individuals. Secondary traumatic stress, like compassion fatigue and vicarious trauma, falls within the category of “empathy-based” stress outcomes for caregivers (Heber et al., 2023).
Scope of Practice: The roles and functions that members of a profession are legislated, educated and authorized to perform and for which they are held accountable.
Therapeutic Modality: A specific method or approach used to treat mental and emotional concerns and to improve mental health. Therapeutic modalities encompass a wide range of techniques and frameworks, each tailored to address different aspects of mental health.
Therapeutic Relationship: A relationship in which the RPN uses their communication skills, understanding of human behaviour and personal strengths to advance the client’s interests, personal growth and the promotion of their health and well-being.
Therapeutic Use of Self: A complex process of self-awareness through one’s own growth and development, as well as one’s interactions with others, that guides the process of developing, maintaining and terminating the therapeutic relationship.
Transference: The client’s experience of feelings toward the RPN that were originally held toward significant others in his or her life (Government of Canada, 2013).
Trauma and Violence-Informed Care (TVIC): An approach that recognizes the widespread impact of trauma and violence on individuals and seeks to create a safe, supportive environment for healing.
Re-traumatization is avoided within TVIC, and the resilience and recovery of those affected by trauma and violence is supported.
Unconditional Positive Regard: Deep genuine caring and acceptance for the client as a person without evaluations, judgements, or stipulations (Corey, 2021).
Vicarious Trauma: Refers to the profound shift in a healthcare professional's inner experience resulting from repeated exposure to a potentially psychologically traumatic event or empathetic engagement with a traumatized person (e.g. learning about another’s trauma or providing professional or personal support or care to a traumatized person). Over time, exposure can lead to changes in the caregiver's perception of themselves, others, and the world, potentially affecting their personal and professional life (Heber et al., 2023; Kim et al., 2022).
American Association of Colleges of Nursing. (2024). Clinical judgment. Retrieved from:
https://www.aacnnursing.org/essentials/tool-kit/domains-concepts/clinical-judgement
Canadian Centre for Occupational Health and Safety. (2024). Hazard and risk. Retrieved from:
https://www.ccohs.ca/oshanswers/hsprograms/hazard/hazard_identification.html
Canadian Interprofessional Health Collaborative. (n.d.). What is collaborative practice? Retrieved from:
https://cihc-cpis.com/about-cihc/what-is-collaborative-practice/
Canadian Mental Health Association. (2019, May). Cohesive, collaborative, collective: Advancing mental health promotion in Canada. Retrieved from:
https://cmha.ca/wp-content/uploads/2021/07/MHP-Full-Paper-FINAL- EN.pdf
Centre for Addictions and Mental Health. (2024). Harm reduction resources. Retrieved from:
Corey, G. (2021). Theory and practice of counseling and psychotherapy (10th ed). Boston, MA: Cengage Learning.
Government of Canada. (2013). What makes Canadians healthy or unhealthy? Retrieved from:
Government of Canada. (2014). Indigenous Peoples and human rights. Retrieved from:
https://www.canada.ca/en/canadian-heritage/services/rights-indigenous-peoples.html
Heber, A., Testa, V., Groll, D., Ritchie, K., Tam-Seto, L., Mulligan, A., Sullo, E., Schick, A., Bose, E., Jabbari, Y., Lopes, J., Carleton, R.N. (2023). Glossary of terms: A shared understanding of the common terms used to describe psychological trauma, version 3.0. Health Promotion Chronic Disease Prevention Canada, 43(10/11).
https://doi.org/10.24095/hpcdp.43.10/11.09
Hedman-Lagerlof, E. & Axelsson, E. (2019). Chapter six - Cognitive behavioral therapy for health anxiety. The Clinician’s Guide to Treating Health Anxiety: Diagnosis, Mechanisms, and Effective Treatment, 79-122. Academic press.
https://doi.org/10.1016/B978-0-12-811806-1.00006-8
Hussein, E.M.T., Olfert, M., & Hakkola, J. (2022). Clinical judgment conceptualization scoping review protocol. Teaching and Learning in Nursing, 17(1), 84-101.
https://doi.org/10.1016/j.teln.2021.10.003
Kellerman, B. (1999). Reinventing leadership. New York, NY: State University of New York Press.
Kim, J., Chesworth, B., Franchino-Olsen, H., & Macy, R. J. (2022). A scoping review of vicarious trauma interventions for service providers working with people who have experienced traumatic events. Trauma, Violence & Abuse, 23(5), 1437–1460.
https://doi.org/10.1177/1524838021991310
Kunyk, D., Peternelj-Taylor, C., &. Austin, W. (2023). Psychiatric and mental health nursing for Canadian practice. Philadelphia: PA: Wolters Kluwer.
McGill University. (2024). Equity, diversity, and inclusion. Retrieved from:
https://www.mcgill.ca/gps/files/gps/equity_diversity_and_inclusion.pdf
Mental Health Commission of Canada. (2016). Guidelines for recovery-oriented practice. Retrieved from:
https://mentalhealthcommission.ca/resource/guidelines-for-recovery-oriented-practice/
Moghabghab, R. T., A. Tong, A. Halloran & J. Anderson. (2018). The difference between competency and competence: A regulatory perspective, Journal of Nursing Regulation. 9(2), 54–59.
Pan American Health Organization (PAHO). (2022). A guide for evidence-informed decision-making, including in health emergencies. Washington, DC: PAHO.
Patel, K. M. & K. Metersky. (2022). Reflective practice in nursing: A concept analysis, International. Journal of Nursing Knowledge. 33(3), 180–187.
Prevention United. (n.d.). What is mental health promotion? Retrieved from:
https://preventionunited.org.au/how-prevention-works/what-is-mental-health-promotion/
Reist, C., Petiwala, I., Latimer, J., Raffaelli, S. B., Chiang, M., Eisenberg, D., & Campbell, S. (2022). Collaborative mental health care: A narrative review. Medicine, 101(52), e32554.
https://doi.org/10.1097/MD.0000000000032554
Robinson, S. (1991). Chapter 15: Collaborative consultation. Learning about learning disabilities. B. Y. L. Wong (Ed.). Academic Press, 441-463.
https://doi.org/10.1016/B978-0-12-762530-0.50021-7
Storey, L. H., J. Howard & A. Gillies. (2018). Competency in healthcare: A practical guide to competency frameworks. London: CRC Press.
Tanner, C. A. (2006). Thinking like a nurse: A research-based model of clinical judgment in nursing. Journal of Nursing Education, 45(6), 204-211.
https://doi.org/10.3928/01484834-20060601-04
Thomas, C. (2021). Taber's medical dictionary. Philadelphia, PA: Davis Company. Retrieved from:
University of British Columbia. (2021). Intersectionality: What it is and why it matters. Retrieved from:
https://vpfo.ubc.ca/news/intersectionality-what-is-it-and-why-it-matters/
World Health Organization. (2010). Framework for action on interprofessional education and collaborative practice. Retrieved from:
World Health Organization. (2024a). Health promotion. Retrieved from:
http://www.who.int/topics/health_promotion/en/
World Health Organization. (2024b). Primary health care. Retrieved from:
https://www.who.int/health-topics/primary-health-care#tab=tab_1